| Sign In | Join Free | My esadidasol.com |
|
| Sign In | Join Free | My esadidasol.com |
|
| Categories | Laryngeal Mask Airway |
|---|---|
| Brand Name: | EasyThru or OEM |
| Model Number: | 1.0# 1.5# 2.0# 2.5# 3.0# 4.0# 5.0# |
| Certification: | CE, ISO13485 |
| Place of Origin: | Nanchang, jiangxi China(Mainland) |
| MOQ: | 100piece |
| Payment Terms: | L/C, T/T, Western Union, D/A, D/P |
| Supply Ability: | 100000piece per month |
| Delivery Time: | 20-35days |
| Packaging Details: | Individually Polybag Packing |
| Price: | Negotiation |
| material: | Silicone |
| Place of Origin:: | Jiangxi, China (Mainland) |
| Sterile: | Yes |
| Usage: | Single-use |
| Feature: | Comfortable |
| Type: | General Medical Supplies |
| Color: | fresh/blue/clear |
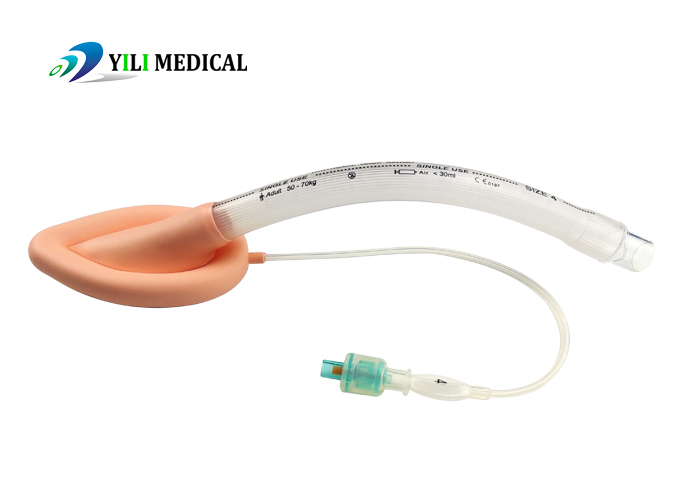
Medical disposable silicone laryngeal mask (LMA) in medical manufacturer with CE/ISO
Features:
1.Made of medica silicone ,have good bicompatibility ,non-toxic.
2.Exclusive soft seal cuff can be insert comforable ,minmizing potential trauma and increasing sealing
3.Strengthen nek and tip eases insertion and prevents folds
4.Kink-free tube eliminates the risk of airway tube occlusion.
5.Have different sizes,suitable for neonate ,infant ,child and adult.
6. Different colors of cuff:blue ,clear ,flesh ,color-coded ballon and connector.
Detail information:
| Ref. No | Description | Size | O.D | I.D |
| YILI-I-1.0 | Neonate <5kg | 1.0 | 9.0mm | 5.4mm |
| YILI-I-1.5 | Neonate/Infant 5-10kg | 1.5 | 10.3mm | 6.1mm |
| YILI-I-2.0 | Infant 10-20kg | 2.0 | 11.5mm | 7.0mm |
| YILI-I-2.5 | Children 20-30kg | 2.5 | 13.3mm | 8.3mm |
| YILI-I-3.0 | Children/Adult 30-50kg | 3.0 | 15.0mm | 10.0mm |
| YILI-I-4.0 | Adult 50-70kg | 4.0 | 15.0mm | 10.0mm |
| YILI-I-5.0 | Adult 70-100kg | 5.0 | 16.5mm | 11.5mm |
Adverse reactions of laryngeal mask airway ventilation
Respiratory obstruction
1) Improper LMA position, folding or rotation of the ventilation
hood, excessive inflation of the ventilation hood, temperature
increase or N2O dispersion increase the volume inside the
ventilation hood and close the glottis.
2) Children have a large tongue, a high and anterior glottis
position, and a large and soft epiglottis that often covers the
pharynx, causing respiratory obstruction. The incidence of
respiratory obstruction in children is nearly twice that of adults.
Reflux, aspiration
1) Anesthesia and surgery significantly reduce the tension of the
upper and lower esophageal sphincters and normal physiological
protective reflexes (coughing, breath holding, etc.).
2) The volume of pediatric gastric juice is relatively large, with
high intragastric pressure and low pH, which poses a relatively
high risk of reflux and aspiration during anesthesia.
3) LMA cannot effectively isolate the esophagus and trachea, and
when factors such as shallow anesthesia, surgery, and coughing
affect it, it is prone to induce reflux aspiration.
Air leakage around the laryngeal mask
1) Poor alignment.
2) The selection of laryngeal mask model is not appropriate.
3) Excessive airway pressure.
4) Implanted too shallow or too deep.
Postoperative sore throat
1) The incidence of throat pain after using laryngeal mask surgery
is very low, with only 7% reported in the literature.
2) Tracheal intubation can reach up to 47%.
3) Mask and oropharyngeal airway can reach up to 10%.
Laryngeal spasm
Reason: Inserting or removing a laryngeal mask under shallow
anesthesia can induce severe laryngeal spasm, leading to negative
airway pressure and lung injury; Stimulation such as surgery or
sputum aspiration can also cause throat reflexes and cause
laryngeal spasms.
Treatment: Generally, relief can be achieved through oxygen
inhalation or deepening anesthesia. For patients with severe
laryngeal spasms who are difficult to inhale oxygen under pressure
with a mask, succinylcholine should be used in a timely manner and
tracheal intubation should be repeated.
Product photo:


|
